Congenital neoplasia
Congenital neoplasia
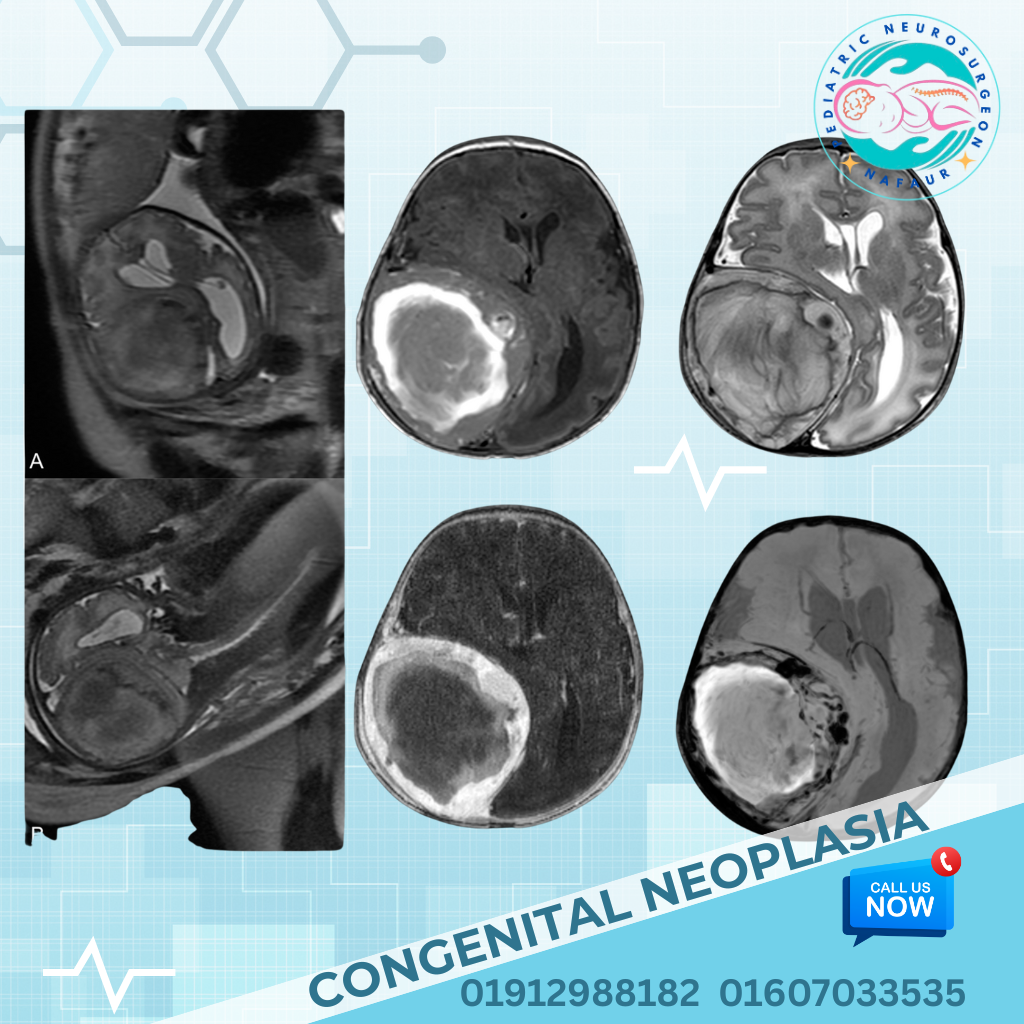
Congenital cranial neoplasia refers to tumors of the brain, skull, or intracranial structures that are present at birth or develop within the first months of life. These tumors are rare but clinically significant, often causing increased intracranial pressure, neurological deficits, or head deformities. They may be benign or malignant, and can arise from a wide range of tissues—glial, neuronal, meningeal, mesenchymal, or germ cell origins. Due to their early onset and location within a developing brain, congenital cranial neoplasms often present unique challenges in diagnosis, surgical management, and long-term prognosis. 🌍 Congenital Cranial Tumors in the Bangladesh Context Many congenital brain tumors in Bangladesh go undiagnosed during pregnancy due to limited availability of fetal anomaly scanning in rural and semi-urban areas Postnatal presentation often occurs late, with enlarged head size, bulging fontanelle, or seizures Cultural misconceptions, lack of early neuroimaging, and limited access to pediatric neurosurgeons delay treatment With improved access to MRI/CT imaging and availability of pediatric brain tumor surgery at NINS and Bangladesh Paediatric Neurocare Centre, early intervention is now possible in major cities like Dhaka 🧠 Common Types of Congenital Cranial Neoplasia Congenital Teratomas Most common; may be intracranial or extracranial Composed of multiple tissue types (hair, teeth, bone, etc.) Often large, cystic, and cause hydrocephalus or skull deformity Choroid Plexus Papilloma Tumor arising from the ventricular system Causes excessive CSF production, leading to hydrocephalus Medulloepithelioma & Ependymoblastoma Highly malignant and aggressive tumors Require early diagnosis and multimodal therapy (surgery + chemo) Congenital Gliomas Astrocytomas or other glial tumors present at birth May be benign or aggressive depending on location and histology Craniopharyngioma (rare congenital form) Often diagnosed in older children but may be present congenitally Congenital Meningioma May arise from dura; typically benign but compress nearby structures Rhabdoid Tumor or ATRT (Atypical Teratoid Rhabdoid Tumor) Extremely aggressive; requires early surgical resection and chemotherapy ⚠️ Symptoms and Clinical Presentation Macrocephaly (enlarged head size) Tense or bulging fontanelle Seizures or abnormal movements Poor feeding, vomiting, or failure to thrive Sunsetting eyes, lethargy Skull deformity or visible mass (especially extracranial teratomas) Developmental delay or regression In some cases, diagnosed via antenatal ultrasound or fetal MRI 🔍 Diagnosis and Evaluation 1. Prenatal Diagnosis Fetal ultrasound (18–22 weeks) may reveal large mass or ventricular dilation Fetal MRI for further characterization (available in limited centers) 2. Postnatal Imaging MRI Brain with contrast – gold standard for identifying tumor type, size, and relation to brain structures CT scan – useful for evaluating calcifications or skull involvement Ultrasound through fontanelle in neonates for bedside screening Tumor markers (AFP, β-HCG) for suspected teratomas or germ cell tumors Histopathological biopsy (after surgical removal or guided needle biopsy) 🛠️ Surgical Management Surgery is the primary treatment for most congenital cranial tumors and must be handled by an experienced pediatric neurosurgical team. Surgical Goals: Safe and complete tumor resection without neurological damage Control of hydrocephalus via VP shunt or ETV if needed Tissue diagnosis for further oncological treatment Preservation of critical neurovascular structures Surgery Types: Craniotomy with microsurgical excision Endoscopic resection for select intraventricular tumors Emergency decompression in life-threatening mass effect CSF diversion procedures for raised intracranial pressure 🧬 Multimodal Therapy and Follow-Up Chemotherapy and/or radiotherapy in malignant tumors (e.g., ATRT, embryonal tumors) Neuro-oncology follow-up for growth monitoring, tumor recurrence Rehabilitation support including physiotherapy, speech therapy, and developmental assessment Lifelong surveillance in some cases, depending on tumor type 🔄 Prognosis Benign tumors (e.g., teratomas, meningiomas) have excellent prognosis with complete excision Malignant tumors may recur despite surgery and require aggressive treatment Early intervention improves chances of normal neurodevelopment, especially if seizures and hydrocephalus are avoided Delayed treatment is associated with poor neurological outcomes 👨⚕️ Why Choose Dr. Md. Nafaur Rahman for Pediatric Brain Tumors? One of Bangladesh’s most experienced pediatric neurosurgeons, with deep expertise in congenital cranial tumors Performs complex neonatal brain surgeries with microsurgical precision at NINS Leads a multidisciplinary team at Bangladesh Paediatric Neurocare Centre for complete neuro-oncological care Offers prenatal counseling, surgical planning, and post-op rehabilitation for optimal child development Trusted by families across the country for safe, compassionate, and effective care 📞 Book a Consultation Today Dr. Md. Nafaur Rahman Assistant Professor, Department of Pediatric Neurosurgery, NINS Chief Consultant, Bangladesh Paediatric Neurocare Centre 📞 For Appointments: 01912988182 | 01607033535 🌐 Website: www.neurosurgeonnafaur.com