Basal Encephalocele
Basal Encephalocele
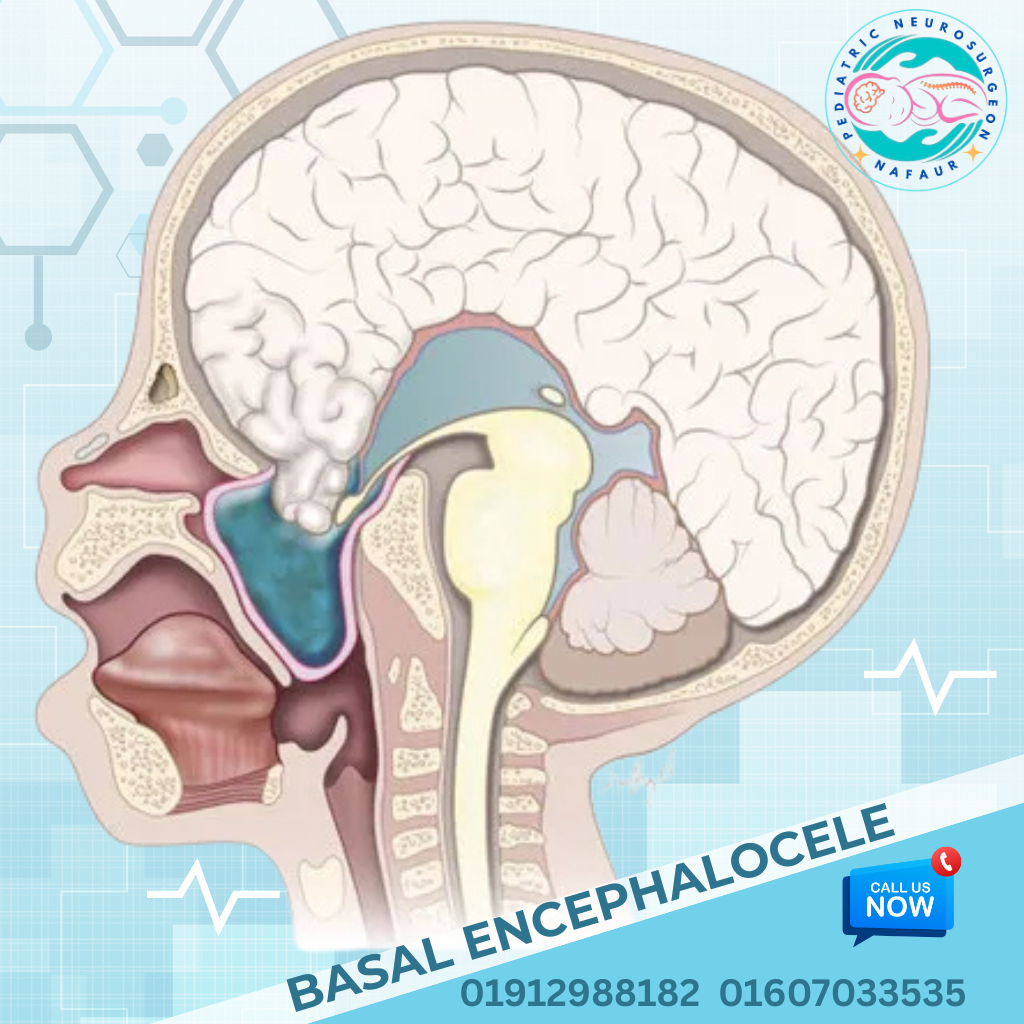
Basal encephalocele is a rare and often hidden form of congenital neural tube defect (NTD) in which brain tissue and meninges herniate through a defect in the base of the skull. Unlike more visible encephaloceles (occipital or frontoethmoidal), basal encephaloceles are often internal, protruding into the nasal cavity, nasopharynx, orbit, or sphenoid sinus. As a result, diagnosis may be delayed unless symptoms prompt early imaging. Basal encephaloceles can cause nasal obstruction, breathing difficulty, vision problems, or cerebrospinal fluid (CSF) leakage, and are often misdiagnosed as nasal polyps or tumors in Bangladesh. 🌍 Basal Encephalocele in the Bangladesh Perspective In Bangladesh, early identification and specialist referral are challenging due to: 🏥 Lack of awareness among primary care and ENT physicians 🔬 Limited prenatal and neonatal MRI/CT access in rural regions 👃 High incidence of misdiagnosis as nasal growths 🧠 Rare presentation leading to delayed pediatric neurosurgery consult ❌ Increased risk of CSF leak, infection, and meningitis due to mismanagement Dr. Md. Nafaur Rahman, with his expertise in complex congenital neurosurgical anomalies, is one of the few specialists in Bangladesh trained to diagnose and surgically treat basal encephaloceles using advanced microsurgical and skull base techniques. 🔍 Types of Basal Encephalocele Basal encephaloceles are classified based on the anatomical skull base defect and herniation path: Transsphenoidal – Through sphenoid sinus into nasopharynx Transethmoidal – Through cribriform plate into nasal cavity Sphenoorbital – Into the orbit, may cause proptosis Sphenomaxillary – Into the maxillary sinus Transclival – Herniating into the posterior pharynx ⚠️ Symptoms and Clinical Presentation Unlike external encephaloceles, basal encephaloceles are not externally visible, making clinical suspicion vital. Symptoms include: 👶 Nasal obstruction or mass in the nasal cavity 💧 Intermittent or continuous CSF rhinorrhea (watery nasal discharge) 🧠 Recurrent meningitis or febrile seizures in infants 👁️ Vision issues or proptosis (eye protrusion) if orbital involvement 🧒 Delayed development or behavioral abnormalities 👃 Difficulty feeding or breathing in neonates 🩸 Nasal bleeding or crusting (if misdiagnosed as tumor or polyp) 🧬 Associated with midline craniofacial defects or cleft palate “Basal encephalocele hides behind the face—but its danger is real. Early diagnosis and safe skull base repair can save a child from a lifetime of complications.” — Dr. Md. Nafaur Rahman 🧪 Diagnosis: Imaging is Essential Due to its hidden nature, accurate imaging is critical for diagnosis and surgical planning: 🧲 MRI Brain with skull base screening – To identify soft tissue herniation 🦴 CT Scan with 3D reconstruction – To define the bony skull base defect 💧 Beta-2 transferrin test – Confirms CSF leak in nasal discharge 📈 Nasal endoscopy – May help localize the defect 🧬 Genetic assessment for syndromic features, if present 🛠️ Surgical Management of Basal Encephalocele Surgical repair is the only definitive treatment to close the defect, prevent infection, and restore cranial stability. Surgery is individualized based on type and location. Surgical Objectives: ✅ Close the skull base defect 🧠 Reposition or remove herniated non-functional brain tissue 🔒 Achieve watertight dural closure to stop CSF leakage 🧬 Preserve vision, olfaction, and breathing functions 🛡️ Prevent recurrence and life-threatening infections Surgical Techniques: 🧠 Endoscopic Endonasal Skull Base Repair (preferred for transsphenoidal/ethmoidal) 🧠 Open Transcranial Approach (for large or complex defects) 🦴 Multilayer grafting with fascia lata, fat, bone, or synthetic materials 🧬 Coordination with ENT and craniofacial surgeons if facial reconstruction is needed ⏳ Surgery is ideally performed as early as possible once diagnosed and child is stable, especially in symptomatic cases. 🏥 Postoperative Care and Follow-Up 🛌 Hospital stay: 5–7 days depending on surgical complexity 💉 IV antibiotics to prevent meningitis 💧 Monitoring for recurrence of CSF leak 🧠 Neuroimaging follow-up and developmental assessment 🧒 ENT and ophthalmology follow-up for associated issues 🧘 Long-term neurocognitive and speech therapy if delays present 🔄 Prognosis and Long-Term Outcome Children with basal encephaloceles, when treated early by a trained pediatric neurosurgeon, can experience: ✅ Resolution of nasal obstruction and CSF leak 🔒 Prevention of future meningitis 👁️ Preservation of vision and cranial nerve function 📈 Normal growth and development in most cases 👨⚕️ Why Trust Dr. Md. Nafaur Rahman? 🧠 Expert in complex skull base and congenital neurosurgery 🏥 Operates at National Institute of Neurosciences & Hospital (NINS) 🛠️ Proficient in endoscopic and open cranial base approaches 👶 Provides holistic pediatric care via Bangladesh Paediatric Neurocare Centre ✅ Recognized for safe, ethical, and multidisciplinary care for rare pediatric brain conditions 📞 Book a Consultation for Safe Basal Encephalocele Repair in Bangladesh Dr. Md. Nafaur Rahman Assistant Professor, Pediatric Neurosurgery, NINS Chief Consultant, Bangladesh Paediatric Neurocare Centre 📱 For Serial/Appointments: 📞 01912988182 | 📞 01607033535 🌐 Visit: www.neurosurgeonnafaur.com
Encephalocele