Holoprosencephaly
Holoprosencephaly
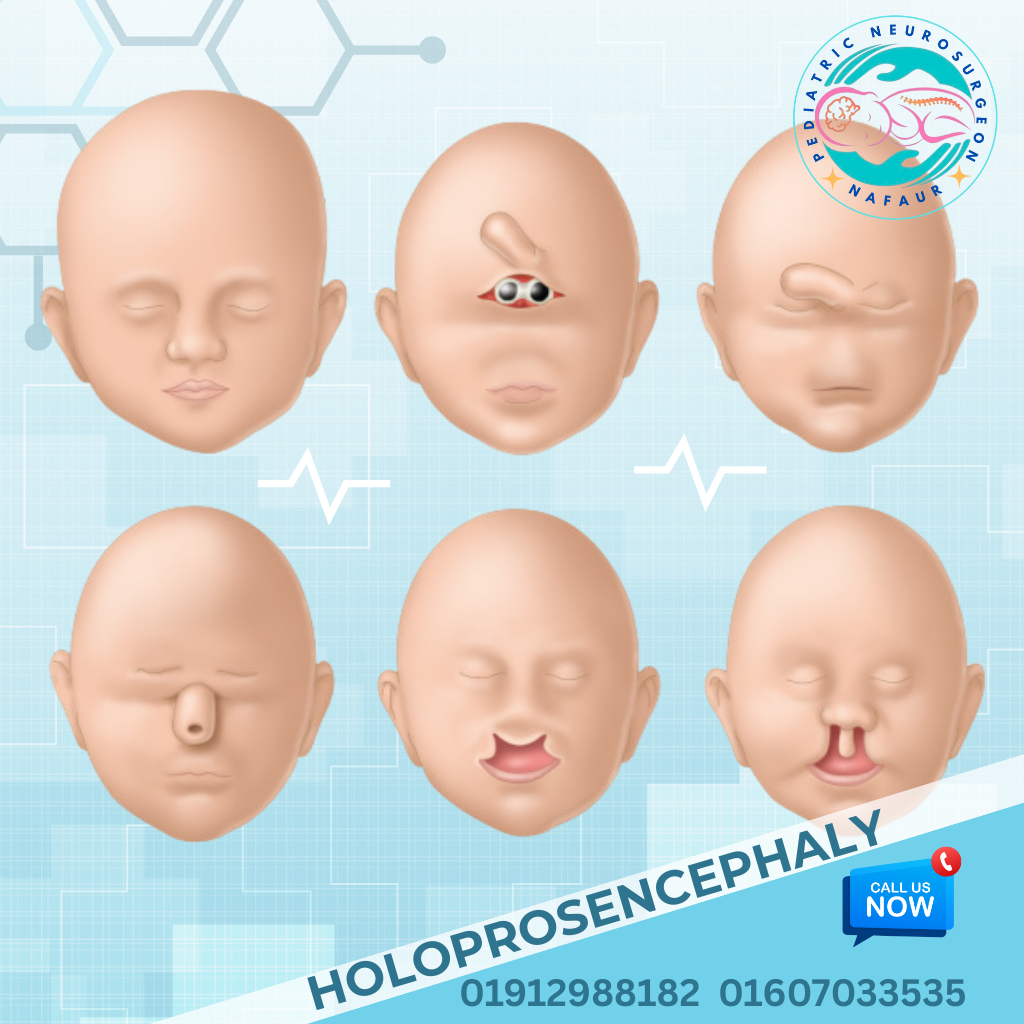
Holoprosencephaly (HPE) is a rare, complex congenital brain malformation in which the developing forebrain (prosencephalon) fails to divide properly into two cerebral hemispheres. This condition arises during early fetal development (between the 18th and 28th day of gestation), resulting in varying degrees of structural brain abnormalities and often facial deformities. Depending on severity, holoprosencephaly is classified into: Alobar HPE – most severe; no separation of cerebral hemispheres Semilobar HPE – partial separation of hemispheres Lobar HPE – milder form with significant brain division but abnormal connections Middle interhemispheric variant (MIH) – partial fusion in the posterior frontal and parietal lobes Holoprosencephaly presents a wide spectrum of clinical manifestations, from incompatible-with-life forms to milder variants allowing long-term survival with neurodevelopmental support. 🌍 Holoprosencephaly in the Bangladesh Context In Bangladesh, most cases are diagnosed late, often during delivery or after onset of severe neurological symptoms There is limited access to early prenatal anomaly scans, particularly in rural areas Many affected families lack awareness about genetic causes, and superstitions may delay proper care Cases often present to pediatricians or neurologists after seizures, facial anomalies, or developmental delay At NINS and Bangladesh Paediatric Neurocare Centre, advanced neurosurgical evaluation, neuroimaging, and multidisciplinary care are available Proper counseling, early imaging, and family education are essential to improve outcomes and planning ⚠️ Causes and Risk Factors Chromosomal abnormalities: Trisomy 13 (Patau syndrome), Trisomy 18 Genetic mutations affecting SHH, ZIC2, SIX3, and other regulatory genes Maternal diabetes, alcohol or drug exposure during early pregnancy Infections during early gestation: CMV, toxoplasmosis, syphilis Nutritional deficiencies, environmental exposures In most cases, the cause remains sporadic or idiopathic 🧒 Signs and Symptoms Clinical presentation varies with the severity of the brain malformation: Neurological Features: Seizures and epileptic spasms Severe developmental delays and intellectual disability Microcephaly (small head size) Hydrocephalus in some cases Spasticity, feeding difficulties, breathing issues Facial Abnormalities: Cyclopia (single eye or closely spaced eyes) in alobar cases Cleft lip and palate Flat nasal bridge, single central incisor Midline facial defects (e.g., hypotelorism) Other: Endocrine abnormalities (e.g., diabetes insipidus, hypothalamic-pituitary dysfunction) Sleep disturbances Gastroesophageal reflux and poor weight gain 🔍 Diagnosis and Imaging Accurate diagnosis requires neuroimaging and multidisciplinary evaluation: Prenatal ultrasound (anomaly scan at 18–22 weeks): can detect severe forms (alobar HPE) Fetal MRI: offers better resolution for planning Postnatal MRI/CT scan of the brain: confirms structural defects and classifies HPE subtype Genetic testing and karyotyping: essential for syndromic or familial cases EEG and hormone panels: assess seizure activity and endocrine status 🛠️ Treatment & Neurosurgical Considerations There is no curative treatment for holoprosencephaly, but neurosurgical and supportive care significantly improve quality of life and survival in mild to moderate cases. Neurosurgical Interventions: Management of hydrocephalus: Ventriculoperitoneal (VP) shunt or Endoscopic Third Ventriculostomy (ETV) Surgical correction of craniofacial abnormalities, such as cleft lip and palate Management of seizures through anti-epileptic medications or surgical evaluation in refractory cases Feeding tube placement or tracheostomy in cases with severe swallowing or respiratory issues Coordination with endocrinologists for hormonal replacement therapy Supportive Management: Physical therapy and occupational therapy Speech and language therapy Nutritional support Developmental stimulation programs Multidisciplinary pediatric care team essential for long-term outcome 🔄 Prognosis and Long-Term Outcome Alobar holoprosencephaly is often fatal in the neonatal period Semilobar and lobar forms may allow survival with significant neurodevelopmental disabilities Cognitive, motor, and speech development is often severely impaired Quality of life depends on the severity, associated anomalies, and access to multidisciplinary care Regular follow-up and early intervention therapies help maximize potential in milder cases 👨⚕️ Why Choose Dr. Md. Nafaur Rahman? Renowned pediatric neurosurgeon in Bangladesh specializing in congenital brain malformations Extensive experience managing hydrocephalus, seizures, and complex neurodevelopmental disorders Operates at NINS, Dhaka — the country’s leading center for advanced neurosurgery Offers family-centered counseling, compassionate care, and modern imaging support Coordinates with pediatricians, geneticists, endocrinologists, and rehabilitation therapists for holistic care 📞 Consult a Pediatric Neurosurgeon for Holoprosencephaly Management Dr. Md. Nafaur Rahman Assistant Professor, Pediatric Neurosurgery, NINS Chief Consultant, Bangladesh Paediatric Neurocare Centre 📞 Call for appointment: 01912988182 | 01607033535 🌐 Visit: www.neurosurgeonnafaur.com