Nasopharyngeal Angiofibromas
Nasopharyngeal Angiofibromas
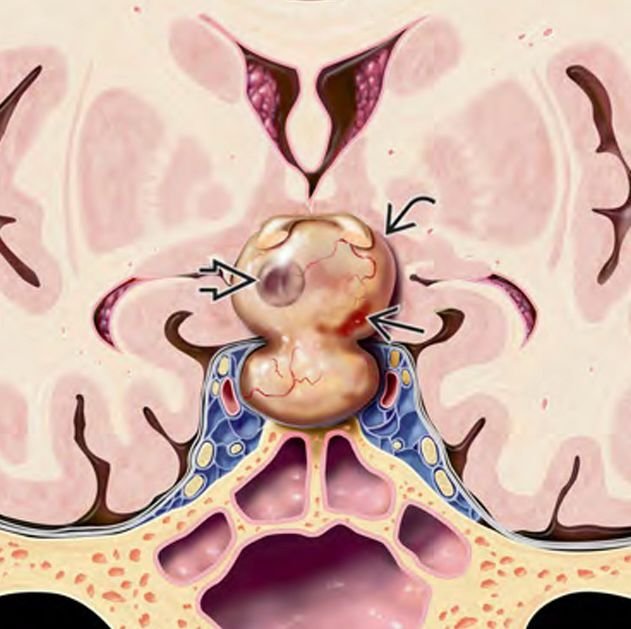
Nasopharyngeal angiofibroma, also known as juvenile nasopharyngeal angiofibroma (JNA), is a benign but highly vascular tumor that arises from the posterolateral wall of the nasal cavity near the sphenopalatine foramen. It predominantly affects adolescent boys, typically between the ages of 10 and 20. Although histologically benign, it can grow aggressively, eroding into the skull base, orbit, and even intracranial space, leading to significant complications. In Bangladesh, delayed diagnosis due to limited awareness, poor access to ENT and neurosurgical services, and financial constraints can cause the tumor to reach advanced stages before intervention. Dr. Md. Nafaur Rahman, a leading pediatric neurosurgeon, offers advanced diagnostic and surgical expertise for managing skull base angiofibromas through minimally invasive and open approaches, with strong emphasis on safety, bleeding control, and functional outcomes. 🌍 Relevance in the Bangladesh Context Juvenile nasopharyngeal angiofibromas are under-recognized in many regions of Bangladesh. Adolescents from rural and semi-urban areas presenting with recurrent nosebleeds, nasal blockage, and facial swelling often go untreated or misdiagnosed until the tumor causes severe complications like proptosis, vision loss, or neurological deficits. Early referral to specialized centers like NINS or the Bangladesh Paediatric Neurocare Centre is crucial to prevent extensive tumor invasion and reduce surgical morbidity. 🧒 Who is at Risk? Adolescent males (10–20 years old) Genetic and hormonal factors may play a role Rarely seen in females or children below 10 years Risk of recurrence if not completely excised 🧠 Symptoms of Nasopharyngeal Angiofibroma Frequent and heavy nosebleeds (epistaxis) – the most common symptom Progressive nasal obstruction Facial swelling or deformity Proptosis (bulging eye) Hearing loss due to Eustachian tube obstruction Headache or facial pain Neurological deficits if tumor invades cranial base Visible mass in oropharynx in advanced cases 🔍 Diagnosis of Skull Base Nasopharyngeal Angiofibroma 🧪 Clinical Evaluation Detailed ENT examination Careful assessment of recurrent epistaxis and nasal congestion 🧠 Radiological Imaging Contrast-enhanced CT scan: Shows bony erosion of skull base, pterygopalatine fossa, and maxillary sinus MRI with contrast: Defines soft tissue involvement, skull base extension, orbital or intracranial invasion MR Angiography or Digital Subtraction Angiography (DSA): Identifies blood supply from internal and external carotid arteries ❌ Biopsy NOT recommended due to risk of massive bleeding 🎯 Classification (Radkowski or Fisch Staging) Stage I: Confined to nasopharynx and nasal cavity Stage II: Extension into sinuses, pterygopalatine or infratemporal fossa Stage III: Skull base or intracranial extension Staging is vital for planning the surgical approach and determining whether embolization is required preoperatively. 🛠️ Treatment Options 1. Surgical Resection The mainstay of treatment Choice of approach depends on tumor size and extent: Endoscopic Endonasal Resection: Preferred for early-stage tumors Open Skull Base Approaches (e.g., transpalatal, lateral rhinotomy, infratemporal fossa approach): For large or invasive tumors Combined Neurosurgical-ENT Approach: For intracranial or orbital extension Dr. Nafaur Rahman utilizes advanced neuronavigation, endoscopic visualization, and intraoperative monitoring to safely remove skull base-invading angiofibromas 2. Pre-operative Embolization Minimizes bleeding during surgery Done 24–72 hours before resection Particularly important in tumors with extensive vascularity 3. Radiation Therapy Reserved for residual or recurrent tumors not amenable to surgery Stereotactic radiotherapy (SRT) or IMRT used cautiously due to long-term risks in growing children 💡 Outcomes and Prognosis Excellent prognosis with complete surgical resection Recurrence rates range from 10–30%, often related to incomplete excision or inadequate imaging Most patients can return to normal life and schooling after recovery Long-term follow-up necessary with serial imaging and nasal endoscopy ⚠️ Complications of Delayed or Incomplete Treatment Life-threatening hemorrhage Permanent cranial nerve deficits Orbital invasion and vision loss Facial disfigurement Intracranial extension causing seizures, hydrocephalus High recurrence if not managed by trained specialists 👨⚕️ Why Choose Dr. Md. Nafaur Rahman? Specialized in pediatric skull base tumor surgeries Works in collaboration with ENT, Interventional Radiology, and Oncology departments Offers minimally invasive and open surgical approaches tailored to patient needs Based at NINS, the top neurosurgical referral center in Bangladesh Provides affordable and evidence-based care at Bangladesh Paediatric Neurocare Centre 📞 Contact for Expert Evaluation Dr. Md. Nafaur Rahman Assistant Professor, Pediatric Neurosurgery, National Institute of Neurosciences & Hospital (NINS) Chief Consultant, Bangladesh Paediatric Neurocare Centre 📞 Serial & Appointment: 01912988182 | 01607033535 🌐 Website: www.neurosurgeonnafaur.com