Bulbar-cervical dissociation
Bulbar-cervical dissociation
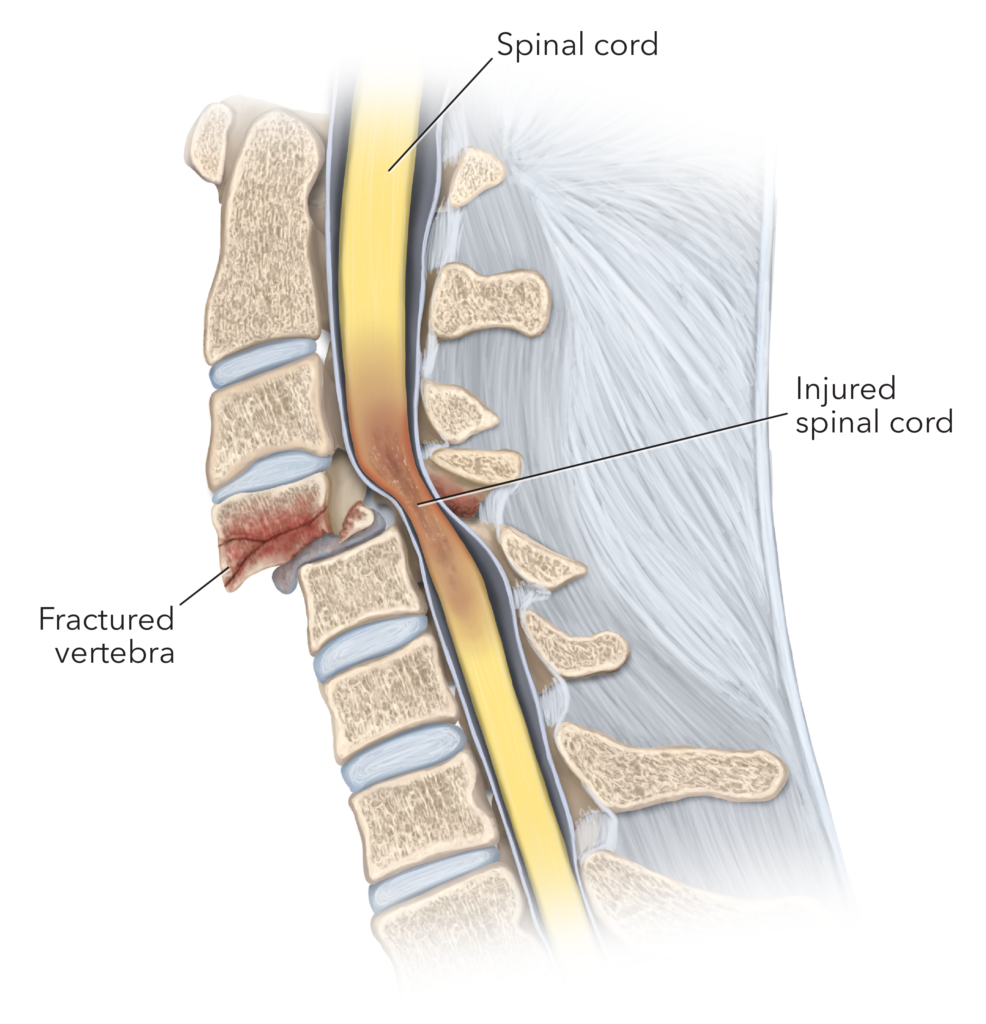
Bulbar-cervical dissociation is a rare and devastating upper cervical spine injury most commonly affecting the craniovertebral junction (CVJ), especially in children. It involves a disconnection between the brainstem (bulbar region) and the cervical spinal cord, often due to high-velocity trauma. This severe form of pediatric spinal cord injury results in immediate disruption of the communication between the brain and the rest of the body. This condition, although uncommon, carries extremely high mortality and morbidity. In countries like Bangladesh, where road safety, fall protection, and emergency trauma care are still evolving, awareness and timely neurosurgical intervention are essential. Pediatric Bulbar-Cervical Dissociation: Bangladesh Perspective In Bangladesh, the number of trauma-related injuries in children is rising due to increased: Road traffic accidents (RTAs) involving motorcycles, rickshaws, and vehicles Falls from rooftops, stairs, or unprotected heights in rural and urban homes High-impact sports or physical abuse (non-accidental trauma) Inadequate use of car seats and helmets for children Unfortunately, due to the silent nature of upper cervical spine injuries, many cases remain undiagnosed or are diagnosed late, leading to irreversible neurological damage or death. Mechanism of Injury Bulbar-cervical dissociation typically results from hyperextension, hyperflexion, or distraction forces that cause: Atlanto-occipital dislocation Ligamentous rupture at the craniovertebral junction Occult fractures of C1, C2 or occipital condyles Complete transection or avulsion of the upper cervical cord Medullary and brainstem disruption Clinical Features Children with bulbar-cervical dissociation present with: Sudden loss of consciousness or coma following trauma Quadriplegia (paralysis of all four limbs) immediately after injury Apnea or respiratory arrest due to involvement of respiratory centers in the medulla Loss of brainstem reflexes, such as pupil reaction, gag, and cough reflex Low or absent blood pressure, indicating neurogenic shock Cardiopulmonary instability This injury is often fatal at the scene or leads to brain death if not identified and managed promptly. Diagnosis Early diagnosis is essential but challenging due to the rarity and rapid deterioration: High-resolution CT scan of the craniovertebral junction to assess bony dislocation or fractures MRI of the craniovertebral junction and upper cervical cord to detect ligamentous injury, cord transection, or hemorrhage Dynamic X-rays (if stable) to detect instability Neurological and brainstem function assessment CT Angiography if vascular injury is suspected In Bangladesh, MRI and CT availability has improved in major urban centers, including Dhaka, under specialized care by pediatric neurosurgeons. Treatment by Dr. Md. Nafaur Rahman Due to the severity of this condition, early stabilization and intensive care support are crucial. Dr. Md. Nafaur Rahman, with extensive experience in managing complex pediatric spine and craniovertebral injuries, offers: Emergency Management Airway and respiratory support, often requiring intubation or mechanical ventilation Hemodynamic stabilization to manage neurogenic shock Immediate immobilization of the cervical spine using pediatric cervical collars or halo vests Administration of high-dose corticosteroids (in selected cases, based on recent protocols) Surgical Management Surgery is often required if the child survives the acute phase: Occipito-cervical fusion (OCF) to stabilize the craniovertebral junction Spinal decompression if compressive hematoma or swelling is present Correction of malalignment using titanium plates, screws, and rods CSF diversion procedures if secondary hydrocephalus or syringomyelia occurs Surgical goals are to stabilize the spine, prevent further neurological injury, and preserve whatever function remains. Prognosis and Outcomes Unfortunately, the prognosis of bulbar-cervical dissociation in children is extremely poor: Many children die at the scene or within 24–48 hours due to brainstem failure Survivors may live in a permanently ventilator-dependent state with complete quadriplegia Early surgical stabilization may help selected children preserve minimal function and improve quality of life Post-operative care includes: Long-term ventilatory support Nutritional support via gastrostomy Bladder and bowel management Neurological rehabilitation if any function remains Pediatric CVJ Injury Care in Bangladesh Dr. Md. Nafaur Rahman is a pioneer in managing pediatric craniovertebral junction injuries in Bangladesh. His team at NINS and Bangladesh Paediatric Neurocare Centre is equipped with: Pediatric-focused ICU care High-resolution imaging Neuro-navigation and spinal instrumentation systems Post-operative neuro-rehabilitation services Contact Dr. Md. Nafaur Rahman 📌 Dr. Md. Nafaur Rahman Assistant Professor, Department of Pediatric Neurosurgery, NINS Chief Consultant, Bangladesh Paediatric Neurocare Centre 📞 For Appointment or Emergency Pediatric Spine Consultation: 📱 +8801912988182 | +8801607033535 🌐 Visit: www.neurosurgeonnafaur.com