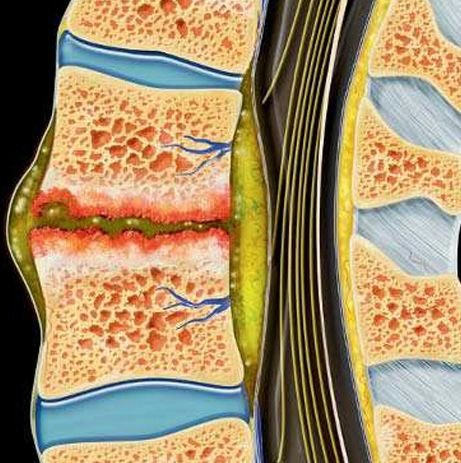
Tuberculous Osteomyelitis
Pediatric Tuberculous Osteomyelitis is a form of skeletal tuberculosis affecting the bones and vertebrae of children, most commonly involving the spine (Pott’s disease). It occurs when Mycobacterium tuberculosis spreads from the lungs or lymph nodes to the bones through the bloodstream. The condition may present subtly with chronic back pain, spinal deformity, or neurological complications due to spinal cord compression.
In Bangladesh, tuberculosis remains endemic, and children are particularly vulnerable due to low immunity, malnutrition, and delayed diagnosis. Dr. Md. Nafaur Rahman leads specialized efforts in early detection, anti-TB therapy, and neurosurgical intervention to prevent permanent disability in affected children.
🌍 Burden of Pediatric Skeletal TB in Bangladesh
Tuberculous osteomyelitis in children is frequently underdiagnosed in Bangladesh due to its slow, non-specific symptoms and resemblance to other infections or orthopedic problems. Key challenges include:
🛌 Lack of awareness among primary caregivers and general physicians
❌ Delayed referral to pediatric neurosurgeons
🔬 Limited access to MRI and TB diagnostic tools in rural regions
🦴 Ignorance of spinal TB signs until deformity or paralysis appears
Dr. Nafaur Rahman’s specialized pediatric neurosurgical practice offers timely diagnosis and comprehensive treatment to prevent long-term damage in children affected by spinal TB.
⚠️ Common Signs & Symptoms
Children may present with a long-standing, low-grade illness often confused with general back pain or fatigue:
🧍 Chronic back pain (especially in thoracic or lumbar region)
😟 Stooping or spinal curvature (kyphosis)
🦵 Weakness or stiffness in the lower limbs
😴 General malaise, weight loss, night sweats
🧑🦽 Neurological symptoms in late stages – numbness, paralysis, bladder/bowel incontinence
🌡️ Low-grade fever persisting for weeks
🛌 Localized spinal tenderness or swelling
“In any child with chronic back pain and low-grade fever in Bangladesh, spinal TB must be suspected early.”
— Dr. Md. Nafaur Rahman
🧬 Causes and Risk Factors
Hematogenous spread of Mycobacterium tuberculosis from a primary site (usually lungs)
Poor immunity due to malnutrition or early childhood TB exposure
Household TB contact (parents, caregivers)
Congenital immunodeficiency
Delayed BCG vaccination or ineffective immunization response
🧪 Diagnostic Approach
Dr. Nafaur Rahman follows an integrated diagnostic protocol with a focus on child-friendly methods:
🔍 Imaging:
🧲 MRI Spine with contrast – Best tool to detect early infection, soft tissue abscess, cord compression
📸 X-ray spine – To detect vertebral collapse or kyphotic deformity
💻 CT scan – Helpful for bony destruction and surgical planning
🔬 Laboratory Investigations:
🩸 ESR and CRP – Usually elevated
🧪 Mantoux test (Tuberculin skin test)
🔍 GeneXpert MTB/RIF – Rapid and specific TB diagnosis
🧬 Biopsy and Histopathology – To confirm TB granulomas, rule out other causes
🧫 Spinal aspirate for AFB stain/culture – If fluid or abscess present
🛠️ Treatment of Pediatric Tuberculous Osteomyelitis
💊 Medical Management:
🛏️ Hospital admission during initial phase
📦 Anti-Tuberculosis Therapy (ATT) – At least 9 to 12 months (4-drug regimen initially)
🎯 Adjusted as per national TB guidelines (e.g., DOTS program)
💊 Pain relief, nutrition, and spinal support with braces
🔧 Surgical Intervention:
Surgery is indicated in:
Progressive spinal deformity (kyphosis)
Spinal cord compression with neurological deficits
Large abscess or cold abscess with compression
Spinal instability or failure of conservative treatment
Dr. Nafaur Rahman performs:
🧠 Spinal decompression and abscess evacuation
🪛 Stabilization with spinal implants in severe collapse or deformity
🧒 Growth-preserving spinal fusion in young children
🔍 Endoscopic or minimally invasive procedures when possible
“Surgical treatment in TB osteomyelitis is not just about infection clearance—it’s about preserving a child’s mobility, growth, and future.”
— Dr. Md. Nafaur Rahman
🔁 Rehabilitation and Long-Term Follow-Up
🧑⚕️ Routine imaging and blood markers to monitor response
🧒 Pediatric physiotherapy to restore posture and gait
🧠 Educational and developmental support
🛡️ BCG vaccination review and household TB screening
🥗 Nutritional rehabilitation for recovery and immunity
🚨 Dangers of Delayed Diagnosis or Incomplete Treatment
🧑🦽 Permanent neurological deficits (paralysis, incontinence)
🦴 Spinal deformity – often irreversible in late stages
⚡ Reactivation of TB or chronic pain
💀 Sepsis or tubercular meningitis in rare complications
🛌 Psychological impact due to long hospital stays and disability
👨⚕️ Why Trust Dr. Md. Nafaur Rahman?
 One of Bangladesh’s top specialists in pediatric spinal tuberculosis
🏥 Practices at National Institute of Neurosciences & Hospital (NINS)
🧒 Experienced in pediatric-friendly surgical techniques
🧠 Skilled in treating both infection and deformity simultaneously
🤝 Trusted across the country for compassionate, ethical, and complete care
📞 Get Help Early – Contact Today
Dr. Md. Nafaur Rahman
Assistant Professor, Pediatric Neurosurgery, NINS
Chief Consultant, Bangladesh Paediatric Neurocare Centre
📱 For Serial/Appointments:
📞 01912988182 | 📞 01607033535
🌐 Website: www.neurosurgeonnafaur.com
One of Bangladesh’s top specialists in pediatric spinal tuberculosis
🏥 Practices at National Institute of Neurosciences & Hospital (NINS)
🧒 Experienced in pediatric-friendly surgical techniques
🧠 Skilled in treating both infection and deformity simultaneously
🤝 Trusted across the country for compassionate, ethical, and complete care
📞 Get Help Early – Contact Today
Dr. Md. Nafaur Rahman
Assistant Professor, Pediatric Neurosurgery, NINS
Chief Consultant, Bangladesh Paediatric Neurocare Centre
📱 For Serial/Appointments:
📞 01912988182 | 📞 01607033535
🌐 Website: www.neurosurgeonnafaur.com